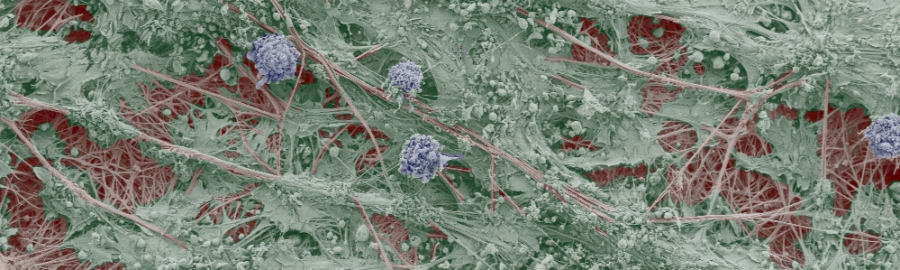
Stem and progenitor cells can be obtained from many different sources, such as the bone marrow, fat, or extra-embryonic tissues. Although stem cells hold great promise for many therapeutic applications, their self-renewal and differentiation characteristics need to be carefully analyzed using adequate in vitro and in vivo models. Due to the absence of phenotypic markers, the isolation of homogeneous population of mesenchymal stem cells (MSCs) from mixed cell populations is not trivial. Furthermore, issues regarding accessibility, tissue-dependent differences in phenotypes and function, tumorigenic potential, and defined differentiation protocols, among others, need to be addressed before these cells can be broadly applied in therapy.
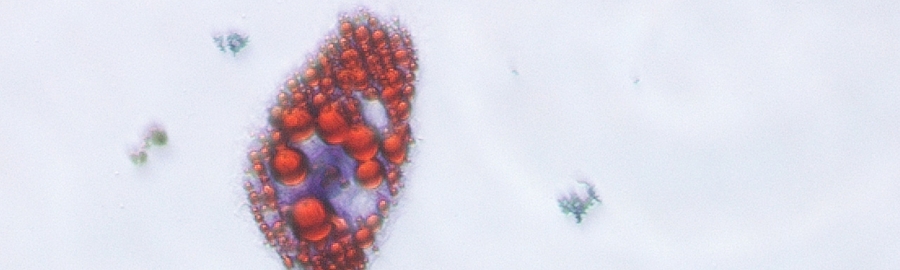
It has been established that amniotic fluid contains stem cells and differentiated cells derived from all three germ
layers. Genome wide analysis of amniotic fluid cells (AFCs)
has shown that they to have a unique stem cell signature and possess characteristics related to pluripotency. Correspondingly their conversion to iPS cells has also been
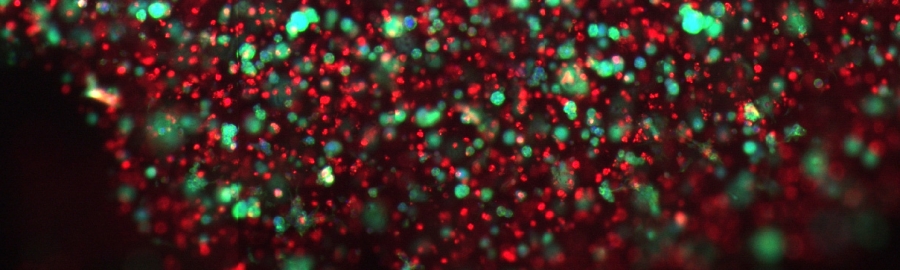
shown to be much easier than of adult cells. In contrast to embryonic stem cells or induced pluripotent stem cells (iPS), AFCs have reduced plasticity and were non-tumorogenic. Clonally expanded AFCs with mesenchymal properties possess large proliferative potential (>250 population doublings) and have been shown to conserve their telomerase activity
up to late passages. Many investigators have also demonstrated the multilineage differentiation capabilities of AFCs, among them conversion to (pre)ostoblasts and endothelial
cells.As amniotic fluid is available without
ethical concerns from routine amniocentesis interventions and might comprise approximately 1% allogeneic stem
cells, it is an attractive cell source, especially for treating congenital disorders in the developing fetus. Using amniotic fluid cells would allow the production of autologous replacement tissues in parallel to the ongoing pregnancy ready to be used for reconstruction when the child is born. In order to standardize the procedure, to improve the engraftment, and to ensure the survival and the function of larger engineered tissue the current project relies on the combination of
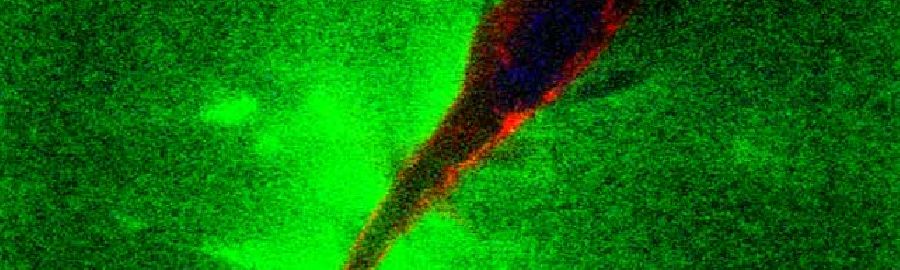
i) the careful characterization of human amniotic fluid derived stem/progenitor cells,
ii) the study of their differentiation potential,
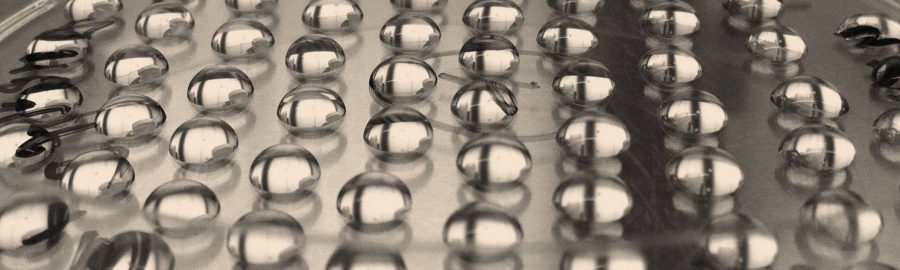
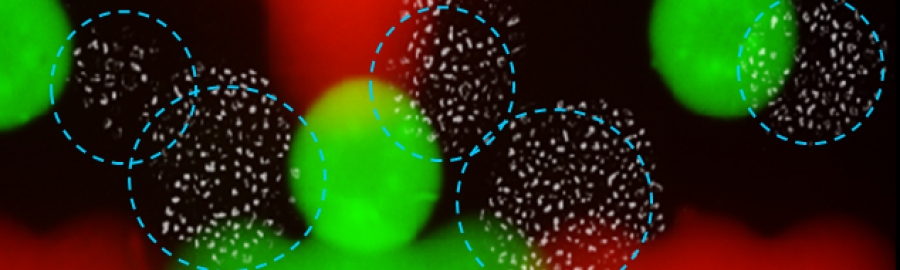
iii) their 3D arrangement using advanced biomaterials technology,
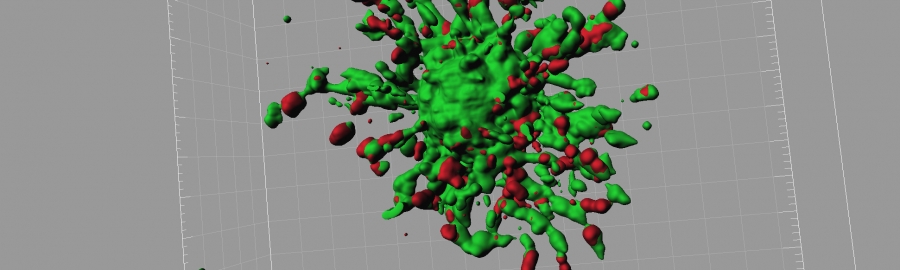
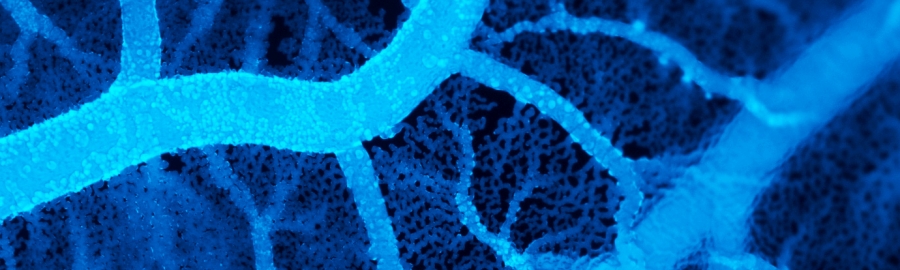
iv) and the formation of pre-vascularized constructs. In contrast to earlier strategies, by this multidisciplinary approach we will be able to form vascularized bone tissues, which will functionally integrate into the existing tissue, representing a breakthrough
for the treatment congenital bone defects.